
Posterior Cruciate Ligament (PCL) Injuries
Introduction - About PCL Injuries
The posterior cruciate ligament (PCL) is one of the less commonly injured ligaments of the knee. Understanding this injury and developing new treatments for it have lagged behind the other cruciate ligament in the knee, the anterior cruciate ligament (ACL), probably because there are far fewer PCL injuries than ACL injuries.
This guide will help you understand
Where the PCL is located
How a PCL injury causes problems
How doctors treat the condition
Where is the PCL, and what does it do?
Ligaments are tough bands of tissue that connect the ends of bones together. The PCL is located near the back of the knee joint. It attaches to the back of the femur (thighbone) and the back of the tibia (shinbone) behind the ACL.
The PCL is the primary stabilizer of the knee and the main controller of how far backward the tibia moves under the femur. If the tibia moves too far back, the PCL can rupture. The PCL is made of two thick bands of tissue bundled together. One part of the ligament tightens when the knee is bent; the other part tightens as the knee straightens. This is why the PCL is sometimes injured along with the ACL when the knee is forced to straighten too far, or hyperextend.
How do PCL injuries occur?
The most common way for the PCL alone to be injured is from a direct blow to the front of the knee while the knee is bent. Since the PCL controls how far backward the tibia moves in relation to the femur, if the tibia moves too far, the PCL can rupture.
Sometimes the PCL is injured during an automobile accident. This can happen if a person slides forward during a sudden stop or impact and the knee hits the dashboard just below the kneecap. In this situation, the tibia is forced backward under the femur, injuring the PCL. The same problem can happen if a person falls on a bent knee. Again, the tibia may be forced backward, stressing and possibly tearing the PCL.
Other parts of the knee may be injured when the knee is violently hyperextended, but other ligaments are usually injured or torn before the PCL. This type of injury can happen when the knee is struck from the front when the foot is planted on the ground.
Symptoms: What do PCL Injuries feel like?
The symptoms following a tear of the PCL can vary. The PCL is not actually enclosed inside the knee joint like the ACL. So unlike an ACL tear, which swells the joint with blood, PCL injuries don't make the knee swell as much.
Most patients with PCL injuries sense a feeling of stiffness and some swelling. Patients may also have a feeling of insecurity and giving way of the knee, especially when trying to change direction on the knee. The knee may feel like it wants to slip. The pain and moderate swelling from the initial injury will usually be gone after two to four weeks, but the knee may still feel unstable.
The symptom of instability and the inability to trust the knee for support are what requires treatment. Also important in the decision about treatment is the growing realization by orthopedic surgeons that long-term instability leads to early arthritis of the knee.
Diagnosis of PCL Injuries -How do doctors identify the problem?
The history and physical examination is probably the most important tool in diagnosing a ruptured or deficient PCL. During the physical examination, the doctor will check to see if the tibia moves too far back on the femur. Tests are also done to see if other knee ligaments or joint cartilage have been injured. The doctor may order X-rays of the knee to rule out a fracture. Ligaments and tendons do not show up on X-rays. T
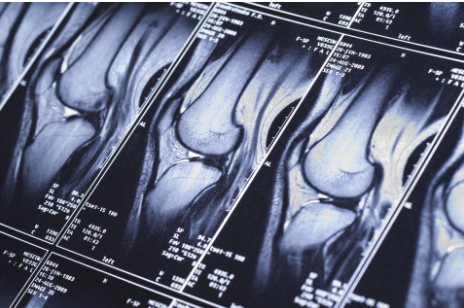
The magnetic resonance imaging (MRI) scan is probably the most accurate test without actually looking into the knee. The MRI machine uses magnetic waves rather than X-rays to show the soft tissues of the body.
This machine creates pictures that look like slices of the knee. The pictures show the anatomy, and any injuries, very clearly. This test does not require any needles or special dye and is painless. In some cases, arthroscopy may be used to make the definitive diagnosis if there is a question about what is causing your knee pain.
Then we have the option of identifying the injury via arthroscopy. Arthroscopy is a type of operation where a small fiber-optic TV camera is placed into the knee joint, allowing the surgeon to look at the structures inside the joint directly. The vast majority of PCL tears are diagnosed without resorting to this type of surgery, though arthroscopy is sometimes used to repair a torn PCL.
Treatment for PCL Injuries
What can be done for posterior cruciate ligament injuries?
Nonsurgical Treatment
Initial treatment for a PCL injury focuses on decreasing pain and swelling in the knee. Rest and mild pain medications, such as acetaminophen, can help decrease these symptoms. You may need to use a long-leg brace and crutches at first to limit pain. Most patients are given the okay to put a normal amount of weight down while walking.
Less severe PCL tears are usually treated with a progressive rehabilitation program. Patients intending to return to high-demand activities may require a functional knee brace before returning to these activities. These braces are designed to replace knee stability when the PCL doesn't function properly.
They help keep the knee from giving way during moderate activity, but they can give a false sense of security and won't always protect the knee during sports that require heavy cutting, jumping, or pivoting. These braces are not the type you can buy at the drugstore. Most orthopedists will recommend wearing a brace for at least one year after a reconstruction, so even if you decide to have surgery, a brace is probably a good investment.
Most patients receive physical therapy treatments after a PCL injury. Therapists treat swelling and pain with the use of ice, electrical stimulation, and rest periods with your leg supported in elevation. Exercises are used to help you regain normal movement of joints and muscles.
Range-of motion exercises should be started right away with the goal of helping you swiftly regain full movement in your knee. This includes the use of a stationary bike, gentle stretching, and careful pressure applied to the knee by the therapist. Exercises are also given to improve the strength of the quadriceps muscles on the front of the thigh.
As your symptoms ease and strength improves, you will be guided in specialized exercises to improve knee stability.
Surgery for PCL Injuries
If the PCL alone is injured, nonsurgical treatment may be all that is necessary. When other structures in the knee are injured, patients generally do better having surgery within a few weeks after the injury. If the symptoms of instability are not controlled by a brace and rehabilitation program, then surgery may be suggested.
The main goal of surgery is to keep the tibia from moving too far backwards under the femur and to get the knee functioning normally again. Even when surgery is needed, most surgeons will have their patients attend physical therapy for several visits before the surgery. This is done to reduce swelling and to make sure you can straighten your knee completely. This practice reduces the chances of scarring inside the joint and can speed your recovery after surgery.
Most surgeons now favor reconstruction of the PCL using a piece of tendon or ligament to replace the torn PCL. This surgery is most often done using the arthroscope (mentioned earlier). Incisions are usually still required around the knee, but the surgery doesn't require the surgeon to open the joint. The arthroscope is used to perform the work needed on the inside of the knee joint. Most PCL surgeries are now done on an outpatient basis, and most patients stay either one night in the hospital, or they go home the same day as the surgery.
In a typical surgical reconstruction, the torn ends of the PCL must first be removed. Once this has been done, the type of graft that will be used is determined. One of the most common tendons used for the graft material is the patellar tendon. This tendon connects the kneecap (patella) to the tibia.
About one-third of the patellar tendon is removed, with a plug of bone at either end. The bone plugs are rounded and smoothed. Holes are drilled in each bone plug to place sutures (strong stitches) that will pull the graft into place. Then holes are drilled in the tibia and the femur to place the graft.
These holes are placed so that the graft will run between the tibia and femur in the same direction as the original PCL. The graft is then pulled into position using sutures placed through the drill holes. Screws are used to hold the bone plugs in the drill holes. Another very common graft involves using two of the tendons that attach to the tibia just below the knee joint, the gracilis, and the semitendinosus tendons.
By arranging these tendons into three or four strips the graft has nearly the same strength as a patellar tendon graft. The gracilis and semitendinosus tendons can be taken out without really affecting the strength of the leg because bigger and stronger hamstring muscles will take over the function of the two tendons that are removed.
Other materials are also used to replace the torn PCL. In some cases, an allograft is used. An allograft is tissue that comes from someone else. This tissue is harvested from tissue and organ donors at the time of death and sent to a tissue bank. The tissue is checked for any type of infection, sterilized, and stored in a freezer. When needed, the tissue is ordered by the surgeon and used to replace the torn PCL. The advantage of using an allograft is that the surgeon does not have to disturb or remove any of the normal tissue from your knee to use as a graft. For this reason, the operation also usually takes less time.
Rehabilitation after PCL Injuries and Surgery
Nonsurgical Rehabilitation
Nonsurgical treatment of an injured PCL will typically last six to eight weeks. You will be able to return to your sports activities when your quadriceps muscles are back to near their normal strength, your knee stops swelling intermittently, and you no longer have problems with the knee giving way. After Surgery You may use a continuous passive motion (CPM) machine immediately after your operation to help the knee begin to move and to alleviate joint stiffness.
The machine straps to the leg and continuously bends and straightens the joint. This continuous motion is thought to reduce stiffness, ease pain, and keep extra scar tissue from forming inside the joint. Your surgeon may also have you wear a protective knee brace for two to three weeks after surgery.
You'll use crutches for two to four weeks in order to keep your knee safe and will probably be instructed to put only a limited amount of weight down while you're up and walking. Patients usually take part in formal physical therapy after PCL reconstruction. The first few physical therapy treatments are designed to help control the pain and swelling from the surgery. Therapists will begin to focus on range of motion exercises within three weeks.
They take care to avoid letting the tibia sag back under the femur, as this can put strain on the healing graft. Strengthening exercises for the quadriceps muscle on the front of the thigh are safe to begin right away. Muscle stimulation and biofeedback, which both involve placing electrodes over the quadriceps muscle, may be needed at first to get the muscle going again and help retrain it. As the rehabilitation program evolves, more challenging exercises are chosen to safely advance the knee's strength and function.
Getting Back to What You Love after PCL Injuries
When you get full knee movement, your knee isn't swelling, and your strength is improving, you'll be able to gradually get back to your work and sport activities. Some surgeons prescribe the use of a functional brace for athletes who intend to return quickly to their sport. Ideally, you'll be able to resume your previous lifestyle activities. However, athletes are usually advised to wait at least six months before returning to their sport. And most patients are encouraged to modify their activity choices. You will probably be involved in a progressive rehabilitation program for four to six months after surgery to ensure the best result from your PCL reconstruction. In the first six weeks following surgery, expect to see the physical therapist two to three times a week. If your surgery and rehabilitation go as planned, you may only need to do a home program and see your therapist every few weeks over the four to six month period.